

1 Introduction
In December 2019, an unprecedented outbreak of pneumonia caused by the SARS-CoV-2 virus, emerged in the city of Wuhan (China). This disease, known as COVID-19, rapidly spread throughout the globe, finding authorities, healthcare providers and lay individuals woefully unprepared, leading to a high degree of uncertainty (Lorettu et al., 2021). By March 2020, many countries had put restrictive measures in place such as lockdowns, curfews, social distancing and quarantines to contain the virus’ spread. These measures had economic and psychological consequences on the people involved (Kunzler et al., 2021; Lima et al., 2020; Nochaiwong et al., 2021; Santomauro et al., 2021; Wu et al., 2021), with some individuals more affected than others (Adams-Prassl et al., 2020; Blundell et al., 2020; Daly et al., 2020). At the same time, the effect of the virus was not uniformly distributed, changing as a function of age and pre-existing medical conditions (Du et al., 2020; Yancy, 2020). As such, the early days of the pandemic presented a stark dilemma to lay-people: how to act for the sake of another in the face of uncertainty, and at what cost? This problem spilled over into socio-political discourse (Barbieri and Bonini, 2020; McKee and Stuckler, 2020; Wolff, 2022) and even prompted acts of violence (Choi and Lee, 2021; Elfrink, 2020; Taylor and Asmundson, 2021). But the pandemic also offered a real-time opportunity to assess costly, individual, pro-social, risky decision-making in instances where even authorities were subject to uncertainty.
1.1 Economic decision-making under risk
Uncertainty has been extensively studied in economic decision-making (Johnson and Busemeyer, 2010; Loued-Khenissi and Preuschoff, 2020; Preuschoff et al., 2013) commonly in the form of “risk,” an expected uncertainty based on event probability. Within this framework, an event is deemed riskier the more unpredictable it is. Hence, high risk differs from predictable danger, which refers to conditions where individuals can easily foresee what will occur. Theoretical and empirical accounts within the domain of economic decision-making (Allais, 1953; Bernoulli, 1738/1954; Cox and Sadiraj, 2008; Tversky and Kahneman, 1992) show that risk steers decision-making away from maximizing predicted gains: agents are risk-averse in the gain domain, showing a preference for sure options, while they are risk-seeking when facing loss. Importantly, risk-seeking decreases linearly with expected monetary loss, a robust phenomenon that has been replicated across different countries (Huck and Müller, 2012; Ruggeri et al., 2020). It remains unclear whether such risk preferences are conserved when deciding for others.
Several empirical studies (Andreoni and Miller, 2002; Cutler and Campbell-Meiklejohn, 2019; Rand and Nowak, 2013) as well as human social structure (Tomasello et al., 2012), provide evidence that other-oriented decisions often violate the homo economicus model (Samuelson, 1993). Individuals commonly engage in costly actions to cooperate with others (Diekmann, 2004; Fehr and Fischbacher, 2004) or to help people in need (Soetevent, 2005), albeit by investing less resources than those usually mobilized for one’s own benefit (Lockwood et al., 2017). Furthermore, several studies have found that decisions made on behalf of others resemble those made for the self (Civai et al., 2010, 2012; Corradi-Dell’Acqua et al., 2013, 2016), thus suggesting an individual ability to put oneself in the shoes of unknown others. When looking specifically at risk preferences, a recent meta-analysis reveals a strong variability in the effects described in the literature, all converging toward an overall trend of slightly enhanced risk-seeking for others relative to one’s self (Polman and Wu, 2020).
1.2 Health decision-making under risk
The role of uncertainty in decision-making also extends to health choices (Reis and Spencer, 2019). In this context, experts, such as authorities or physicians specifically trained in assessing risk, are usually those tasked with making decisions. For instance, authorities may rely on the Precautionary Principle, assuming a risk-averse stance toward public health (Goldstein, 2001; Gollier and Treich, 2003; Sunstein, 2005). Other health evaluations commonly use expected utility (Abellan-Perpiñan et al., 2009; Evans and Viscusi, 1991; Levy and Nir, 2012; Meltzer, 2001; Russell and Schwartz, 2012). For example, the Quality-Adjusted Life-Years (QALY) is a form of expected utility integrating time that guides cost analysis (Bleichrodt, 1997) and health policy implementations (Mooney, 1989; Pinto-Prades et al., 2019). With both the Precautionary Principle and QALYs, the calculus employed in the service of making a decision is explicit. However, the novelty and virulence of Sars-Cov-2 imposed the burden of costly decision-making on people’s health under uncertainty on lay people, leaving the question open as to what strategy is used in such a context. Tversky and Kahneman (1981) speculated that individuals would be risk-seeking for treatment when facing an infectious disease, mirroring choice behavior when facing monetary loss. However, whereas some studies investigating pain-management choices confirm this prediction (Loued-Khenissi et al., 2022), others show that individuals are risk-averse for their own treatment options (Hellinger, 1989) or for choices that could influence their life expectancy (Attema et al., 2013). Finally, meta-analyses suggest that health decision-making in medical contexts lead to a shift toward more cautious (risk-averse) decisions for others relative to the self, in contrast to what is found in monetary/managerial scenarios (Atanasov, 2015; Polman and Wu, 2020). However, the medical contexts included in these meta-analyses involved primarily physicians (or people acting as physicians) choosing for patients (Atanasov, 2015; Polman and Wu, 2020), thus still focusing on decision-making processes in professionals, rather than the lay individual. To the best of our knowledge no studies have tested how ordinary people make risky decisions on disease treatments for unknown others.
1.3 The present research
Here, we investigated uncertainty’s role in costly decision-making for people’s health by applying an expected value model of disease severity in a probabilistic task. We administered two anonymous surveys to the general population between May and July, 2020, when at least half the global population was under confinement and grappling with questions on how to personally respond to the COVID-19 pandemic and how much to sacrifice in service of the greater good. We presented respondents with fictitious diseases and their associated risks of contraction, along with different, costly treatment options. Participants were asked to choose between a treatment that avoids contracting the disease at a given probability (risky option) or one that mitigates symptoms with 100% effectiveness (sure option). Building on a well-established literature from economic decision-making (Johnson and Busemeyer, 2010; Loued-Khenissi and Preuschoff, 2020; Preuschoff et al., 2013), we define a treatment as riskiest when outcome (negatively or positively valenced) probability approached 0.5. Respondents made decisions for themselves (Self), a loved one (Beloved), and a Stranger. In this design, the Self condition represents the baseline against which we compare choices made for others (either the Beloved or a Stranger). In particular, choices made for an unknown person (relative to one’s self) are of key interest, as they provide a snapshot on individual, costly, risky decisions for a stranger’s wellbeing. We included a loved one as a target to further characterize self-other differences, and to investigate effects related to the social proximity of the deciding agent. Following the literature reviewed above, we sought to test the following three hypotheses. First, we expect that, in the Self condition, individuals would display an overall risk-seeking stance that progressively declines with increasing expected disease severity (Hypothesis 1). This prediction is directly derived from studies arguing that choices on disease contraction mirror those observed for monetary losses (Tversky and Kahneman, 1981). Second, we predict that decisions for strangers would be more risk-averse than those associated with the self (Hypothesis 2). This is motivated by previous studies meta-analyses testing risk decision-making in medical contexts (Atanasov, 2015), and pain management (Loued-Khenissi et al., 2022). Third, and consistent with our prior research (Loued-Khenissi et al., 2022), we expect social proximity between self and other to influence the results, with agents acting for their loved ones as they would for themselves (Hypothesis 3).
2 Survey 1
2.1 Methods
2.1.1 Population
The survey was made available online to individuals 18 years and older. Respondents were recruited through the Prolific.co platform. Participation was voluntary and compensated between £1.5 and £2 (i.e., £5/h on an average completion time of 22 min). The Ethics Committee of the Faculty of Psychology and Educational Sciences of the University of Geneva approved the study.
Survey 1 was an exploratory investigation to obtain a first snapshot of decision-making for others’ well-being. Within a week (in May 2020), 381 participants in the Prolific.co platform began the survey, and 366 completed the questionnaire. We excluded an additional 22 participants for making attentional errors (see data analysis below for more details) or providing implausible answers (e.g., listing a non-human as a loved one), leaving n = 344 for analysis [43% F; mean age 25 (IQR = 10)]. Cohort characteristics are described in Table 1.
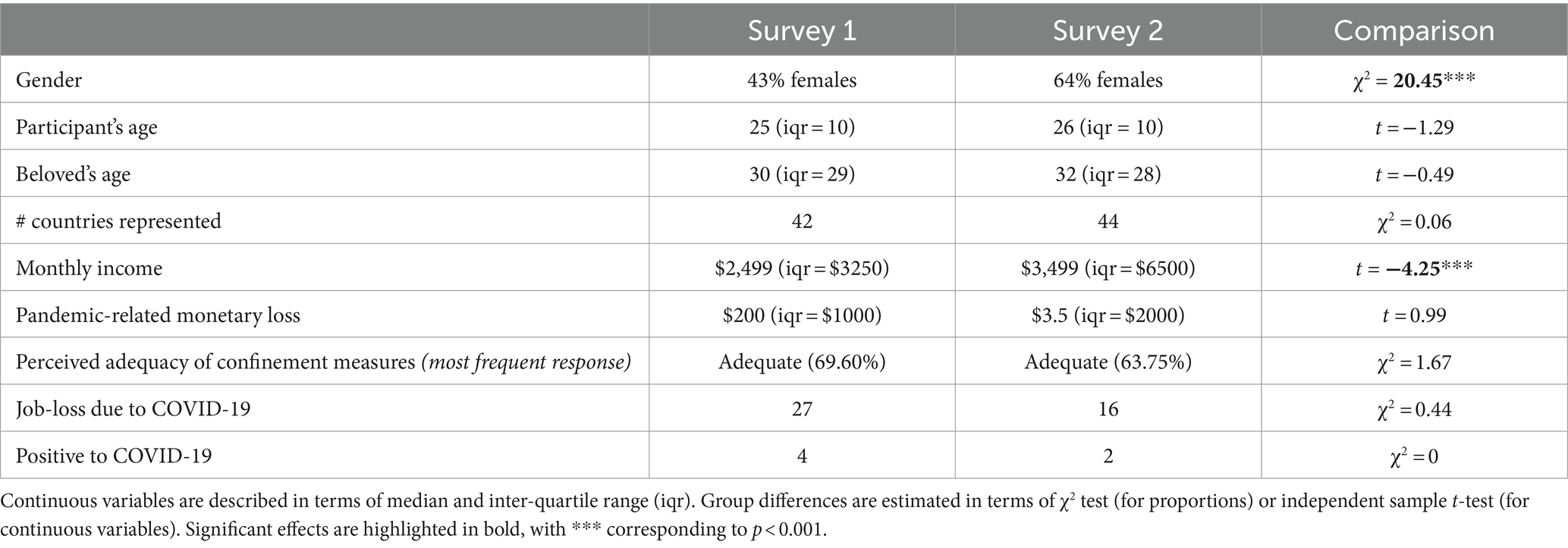
Table 1. Surveys 1 and 2 cohort details.
2.1.2 Procedure
As a first step, participants accessed an informed consent page. By selecting the option “I accept,” they were then directed to the main survey. This was an adaptation of standard lottery tasks from economic decision making (e.g., Tversky and Kahneman, 1992) to the context of a pandemic, where respondents had to choose between different treatments that could either dampen or cure disease at given effectiveness rates. We specifically chose scenarios involving treatments for fictitious diseases, so as to freely manipulate probabilities in a plausible fashion. This manipulation would not have been possible had we employed real diseases (which participants might have prior knowledge of), or non-pharmacological protective behavior like wearing masks or abiding to self-confinement (for which precise probabilities might have appeared implausible). The survey contained 45 items, each describing a risk of contracting a given disease. For each item, respondents chose one of 3 treatment options. Below is an example:
“Your loved one has a 25% chance of contracting and falling severely ill with disease F. Symptoms include high fever, muscle pain and vomiting of blood. Standard treatment requires a two-week hospital stay in intensive care. The illness leaves minor but lasting cardiac deficits and a slight but permanent hearing impairment. You can:
• Do nothing and let your loved one face the initial chance of falling severely ill with disease F
• Pay half your monthly salary for additional treatment that will certainly reduce the severity of the illness, such that it leaves only a slight but permanent hearing impairment
• Pay one tenth of your monthly salary to halve the risk of contracting the illness altogether with an experimental treatment.”
The scenarios described 5 possible diseases, with different risks of contraction (pD; in the example above, 0.25), and levels of severity (SD; either death or severe lasting deficits). Diseases were also described according to their symptoms, which were loosely based on real world infectious diseases (C for Chikingunya; D for Dengue; E for Ebola; F for Flu, etc.), with, however, fictitious morbidity and mortality rates. Each item threatened one of three possible targets (Self, Beloved, or Stranger), and were followed by 3 possible options:
• Do nothing and let the person face the initial risk of disease;
• Pay an amount of money for a known treatment that partially reduces disease severity (sure option);
• Pay an amount of money for an experimental treatment that reduces the risk of initial contraction (the gamble).
The gamble cost was always set to one tenth of the respondent’s monthly income. Sure treatment options for each disease varied in price, between 0.1, 0.5, or 1 unit of the respondent’s monthly income. Selecting the sure option treatment for diseases with a mortal risk (C, D, and E from Table 2) reduced prognosis to severe lasting deficits. Known treatment reduced prognosis to mild lasting deficits for diseases that carried severe lasting deficits (F and M) (see Table 2). Four attentional catch questions were interspersed across the survey to ensure respondent engagement (e.g., “Is 7 > 3?”). All items were randomized across diseases and targets.
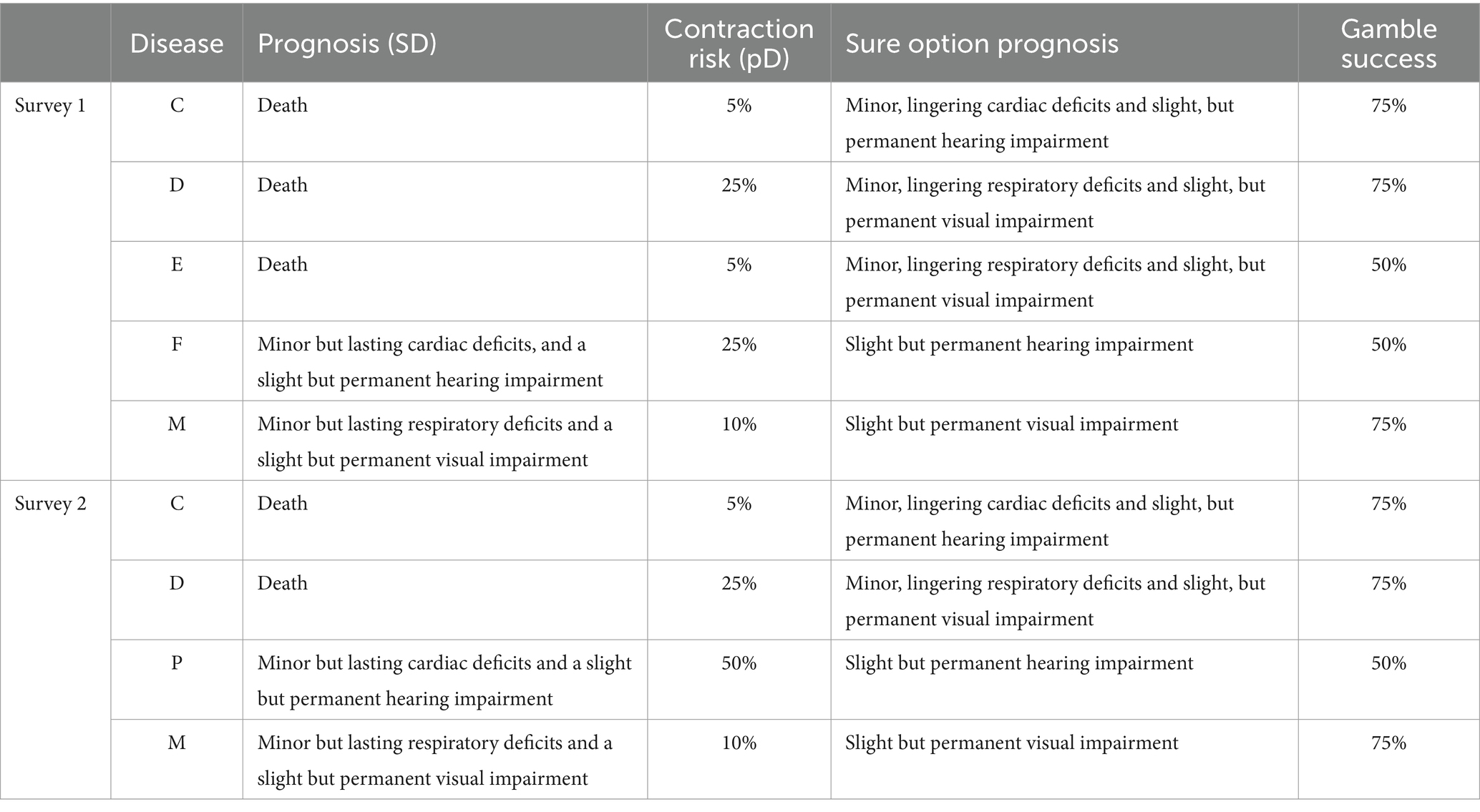
Table 2. Disease items and treatment options.
We also collected participants’ non-identifying demographic information (country of residence, age and gender, and household monthly income and education), that could impact costly, pro-social decision-making (Boschini et al., 2018; Freund and Blanchard-Fields, 2014; Wiepking and Breeze, 2012). We also asked participants to identify a loved one (Beloved) by their role. The survey was designed using LimeWire software, and was fully anonymous; and available in English, French and Italian (English version available under the Open Science Framework
2.1.3 Data analysis
Analyses were performed using R 4.1.2 freeware software; de-identified data and processing scripts are available at:
2.1.3.1 Expected (dis)utility of disease and risk preferences
We modeled responses to disease vignettes using expected utility theory. Specifically, we computed the expected value of disease and associated treatment options to address the main question of decision-making under risk. Each illness presented an expected disutility of disease severity (EDS), computed from the expected utility theorem (Bernoulli, 1738/1954) as follows:
where pD is the probability of contraction and SD is disease severity. Each disease has a specific pD (ranging from 0.05 to 0.50, see Tables 1, 2). SD is a value on an ordinal scale ranging from 1 to 3, where 3 = death; 2 = severe lasting deficits and 1 = minor lasting deficits (the latter case was never used as a starting value, but only as the outcome of the sure option treatment).
2.1.3.2 Linear models
We analyzed participants’ choices using a generalized linear mixed model with binomial distribution and Laplace approximation, to examine factors influencing decisions. First, we assessed the likelihood of making a costly choice (either certain or gamble) as opposed to inaction (Model 1a). Subsequently, we assessed, among costly choices, the likelihood of selecting a gamble over a sure option (Model 1b). In both models, we specified EDS, the sure option’s Price (0.1, 0.5 and 1 unit of monthly income), disease Target (Self, Beloved and Stranger), and the interaction thereof, as fixed factors. EDS and Price were specified as continuous predictors, whereas Target was treated as a categorical factor with three levels. Finally, we designed a linear mixed model to fit the treatment cost (i.e., the chosen treatment prices) as a function of the fixed factors EDS, Target and their interactions (Model 1c). In all three models, participant identity was specified as a random factor, with random intercept and slope for all within-subject predictors. In modeling the random components, we always chose the most complex random structure (slope of simple effects and high order interactions), except in cases of misconvergence, where a simpler structure was adopted (full details on the models implemented are provided in Supplementary Table A1). The analysis was performed using the lmerTest package of R (Kuznetsova et al., 2017).
2.2 Results
2.2.1 Choice analysis
Overall, costly actions were significantly more frequent than inactions [76.53%, 26.67 interquartile range (IQR); test against 50%: t(343) = 25.47, p < 0.001]. This effect was driven by Self and Beloved conditions, where costly actions were chosen most often (88.06%, IQR: 13.33 and 93.72%, IQR: 6.66, respectively). When choosing for a stranger (Other condition), costly options were selected less often, ~47.81% (IQR = 87.67; t(343) = −1.03, p = 0.300; see Figure 1A). Among costly actions, participants preferred gambles (56.04%, IQR: 40.96; t(341) = 4.25, p < 0.001). This effect was driven by Self and Other conditions, where gambles occurred 56.00% (IQR: 51.83) and 71.50% (IQR: 45.63) of the time, respectively. For the Beloved, gambles were chosen ~48.22% (IQR: 50.26; t(340) = −1.10, p = 0.273) of the time.
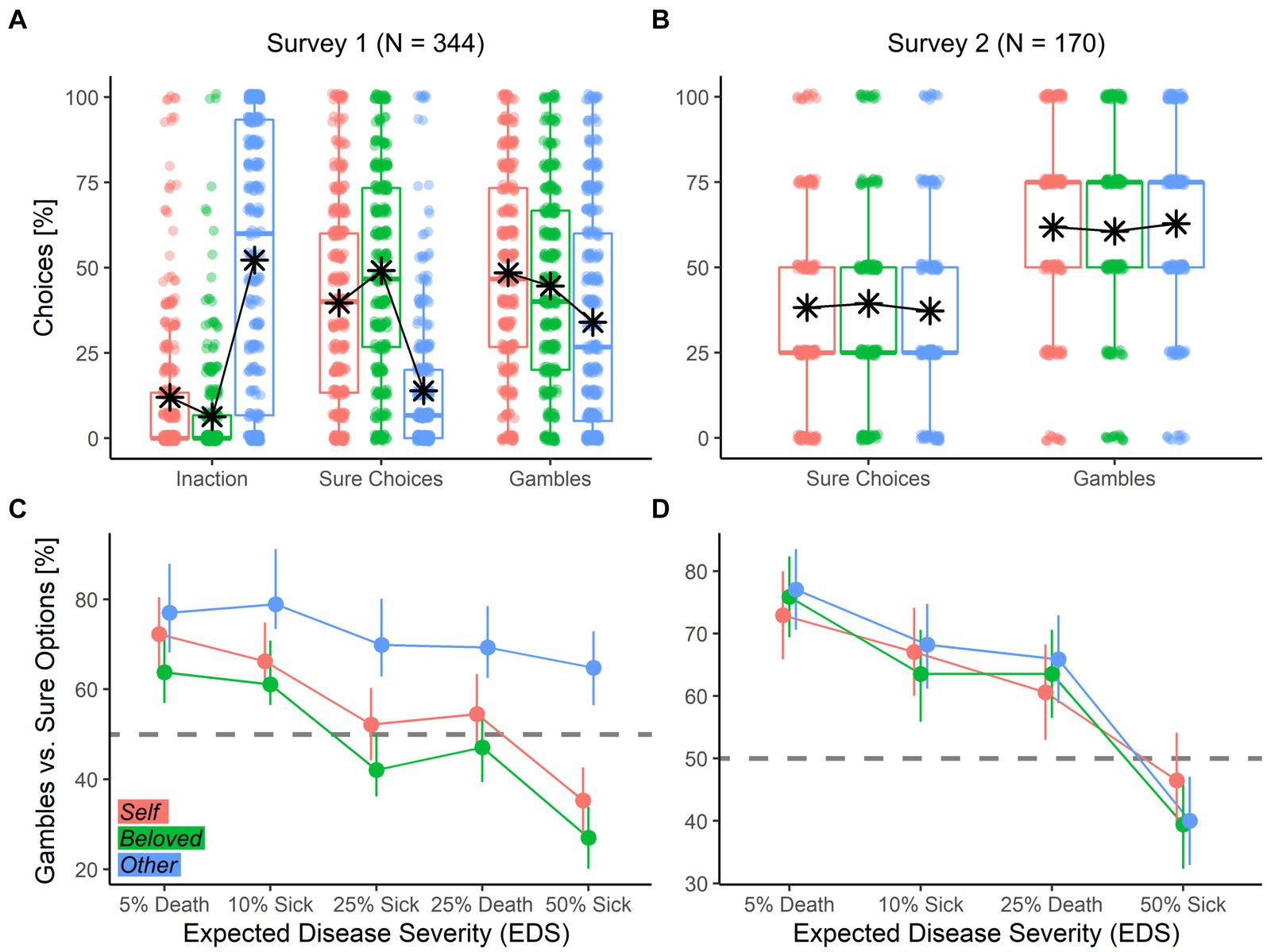
Figure 1. (A,B) Boxplots describing the percentage of each kind of choice across decision targets. For each boxplot, the horizontal line represents the median value of the distribution, the star represents the average, the box edges refer to the inter-quartile range, and the whiskers to the data range within 1.5 of the inter-quartile range. Individual data-points are also displayed as dots. (C,D) Line-graphs describing the relative percentage of Gambles vs. Sure Options across EDS and Target. Each condition is represented by the overall mean with bootstrap-based 95% confidence intervals. The horizontal dashed gray line shows the indifference point.
We extended our analysis in a generalized linear mixed model with a binomial distribution to assess factors affecting choice (Model 1a; Model 1b; Table 3). First, we found a positive effect of EDS on costly (Model 1a) and sure choices (Model 1b) (see Figure 1C; Table 3). We also found an effect of Price, with preferences for the cheaper option (Inaction in Model 1a; Gambles in Model 1b) as the sure option’s price increased; and an effect of Target, with fewer costly (Model 1a) and sure choices (Model 1b) made for the Other (see Figures 1A–C). In Model 1b, when participants chose a costly option, they gambled less for the Beloved. Finally, the three factors of interest interacted with one another, suggesting EDS and Price effects were conditioned on the Target. To further explore these interactions we repeated the previous models in each Target separately (Figure 2). Results confirm both EDS and Price influence self-regarding decisions in opposite directions. Whereas EDS promotes costly (Model 1a) and sure (Model 1b) choice selection, Price promotes inaction and gambles (Figure 2, left column). Price influences decisions for the Beloved less (Figure 2, middle column) while decisions for the Other are less influenced by EDS and more by Price (Figure 2, right column).
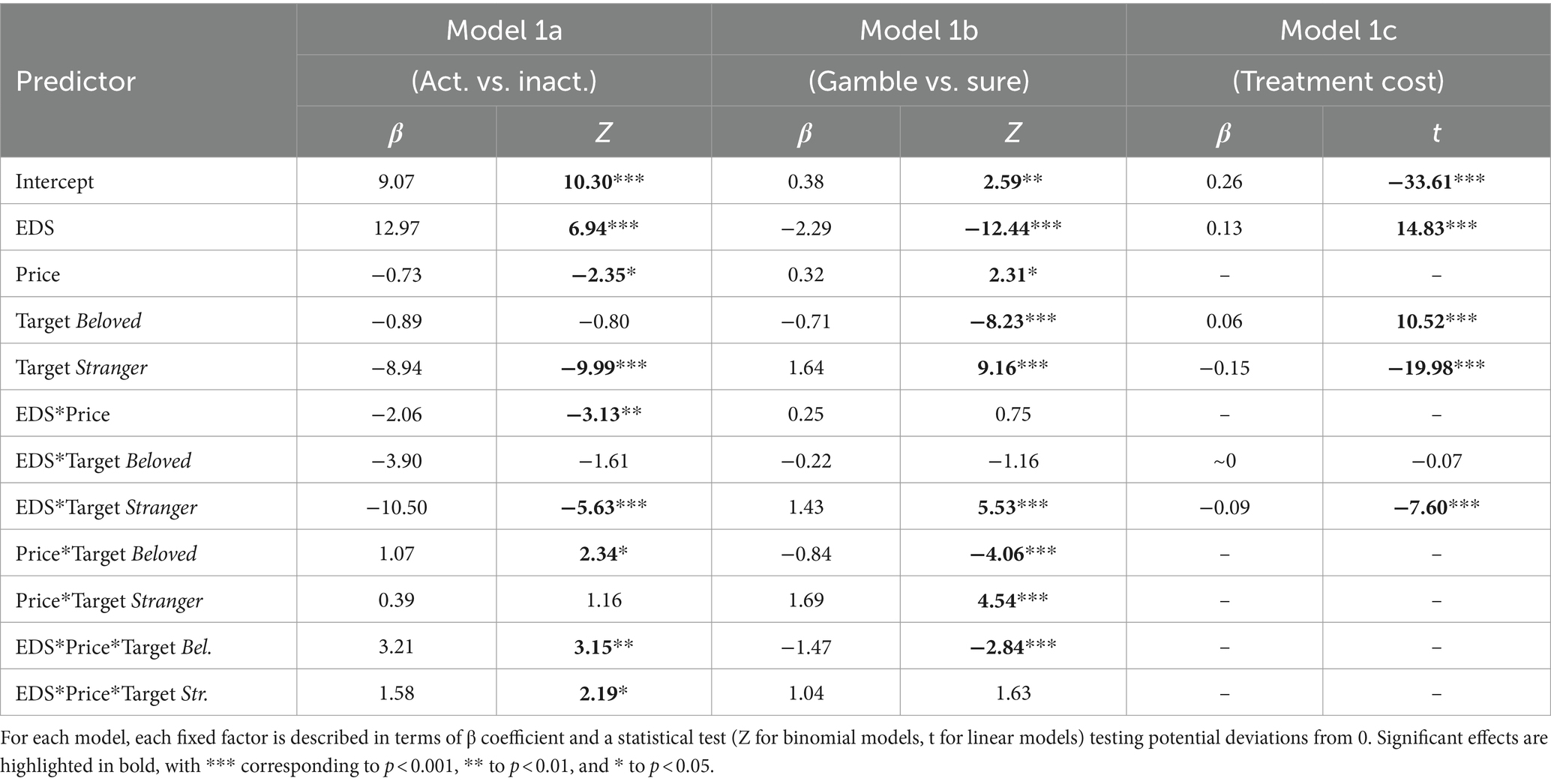
Table 3. Results of Survey 1.
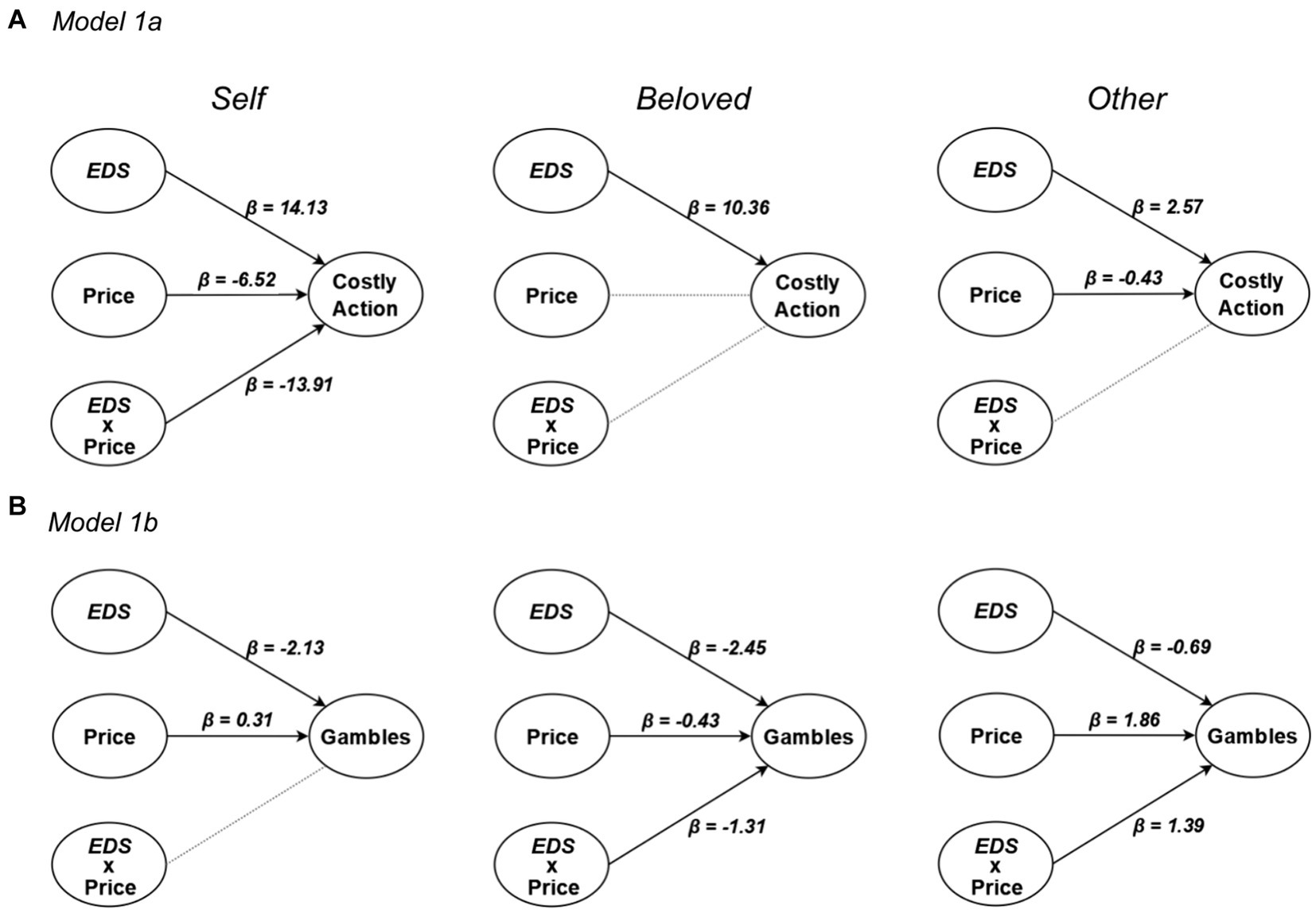
Figure 2. Results from simplified versions of (A) Model 1a and (B) Model 1b for Self (left), Beloved (middle) and Stranger (right) conditions. Significant effects are highlighted as full arrows associated with the corresponding β coefficient from a generalized linear mixed model with binomial distribution. Non-significant effects are displayed as dotted lines.
2.2.2 Chosen treatment price
In a follow-up model, the cost of the selected option was modeled as a dependent variable. Results (see Table 3 and Figure 3A) confirmed that participants spent more on the Beloved, but less on the Stranger. Furthermore, participants spent more for high EDS across targets, but this effect was less pronounced for the Stranger.
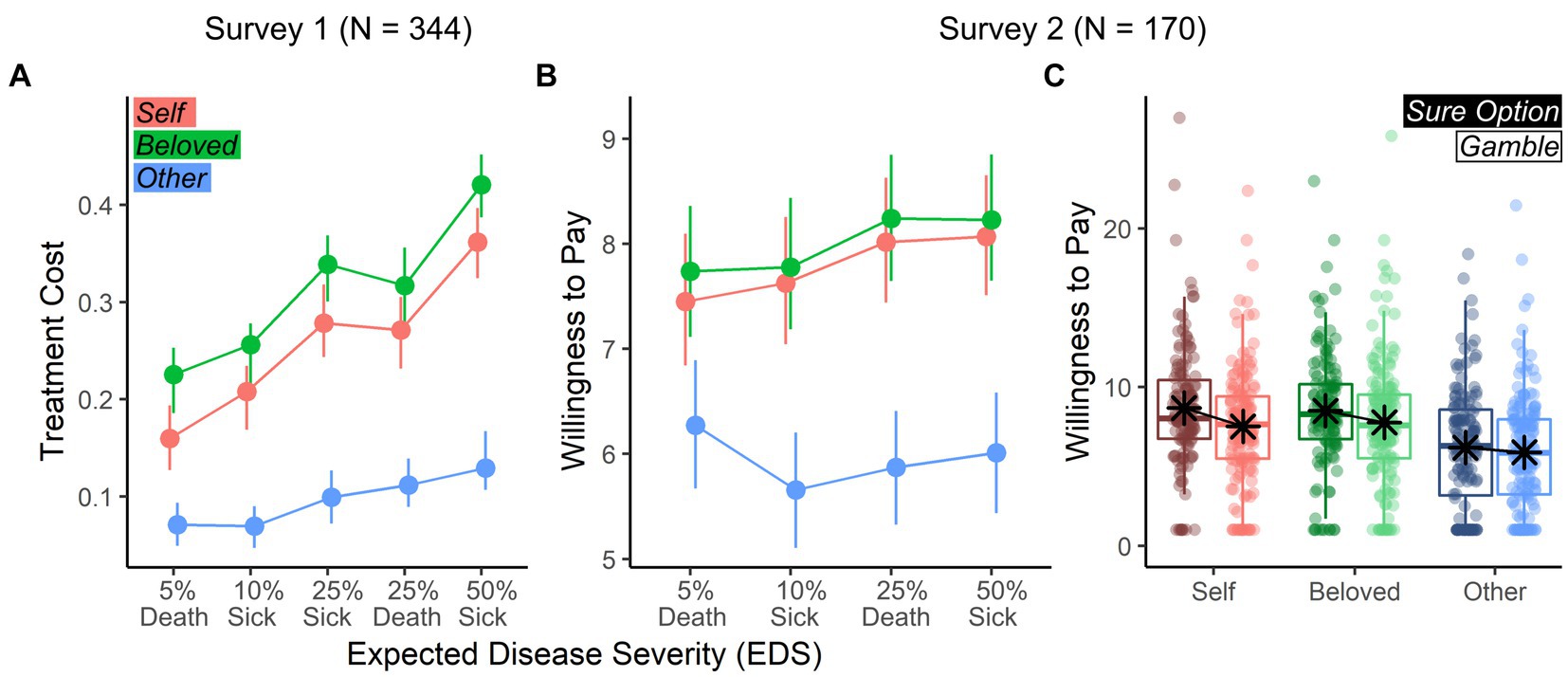
Figure 3. Treatment cost and willingness to pay. (A) Survey 1: Line-graphs describing the average cost (and bootstrap-based 95% confidence intervals) of the chosen treatment across EDS (horizontal axis) and Target (different color-coded lines). Costs are described as proportions of participants’ monthly salary. (B) Survey 2: Line-graphs describing the average willingness to pay of the chosen treatment described as log-transformed USD units. (C) Survey 2: Boxplots describing the willingness to pay across Target and previous choice. Values (in log-transformed USD) are displayed in different colors (to discriminate Targets) and luminance (to discriminate Choice).
2.2.3 Follow-up analyses
2.2.3.1 Nuisance variables
We repeated all above analyses by accounting for Sex, Age, Monthly Income and COVID-19 information (e.g., log-transformed USD financial loss) as nuisance variables. Results confirm effects observed in the main analysis (Supplementary Table A2). We also found a significant effect of Sex, where males chose gambles less frequently (Model 1b) and accepted higher treatment prices (Model 1c).
2.2.3.2 Alternative approach to EDS
All analyses reported were performed by modeling the predictor EDS, an adaptation of expected utility theory to health-based decision-making. In particular, EDS is defined as the product of the probability of contraction (pD) with disease severity (SD), where the latter is treated as a ratio-value although resulting from an ordinal predictor (e.g., 3 = death; 2 = severe lasting deficits and 1 = minor lasting deficits; Methods). As it could be argued that imposing linearity on SD biases the analysis, we repeated the main analyses above, this time modeling the severity of disease as pD + SD, as two independent predictors. Here, pD was specified as a continuous predictor, and SD as a categorical factor (in all diseases, initial SD is either 2 or 3). Full results are displayed in Supplementary Table A3, and reveal that the effects originally attributed to EDS are now associated with pD. In some instances (albeit non-systematically) participants’ choices were also influenced by SD.
2.3 Discussion
This survey tested individual risky decision-making on other’s health using an expected disutility of disease framework. We found evidence supporting Hypothesis 1 as individuals prefer gambles in the disease domain overall, with this preference decreasing linearly with expected severity of disease. This prediction was confirmed by our data (Figures 1A–C, rose data-points), similar to what found in the economic loss domain (Tversky and Kahneman, 1981) and pain management (Loued-Khenissi et al., 2022). More specifically, EDS and treatment price heavily influenced participants’ choices: whereas a disease of higher expected severity increased sure option selection, higher treatment cost increased gamble selection. Our prediction that individuals would be more risk averse for unknown others (Hypothesis 2) was not observed in our data, as participants selected sure options less frequently when acting for the Stranger (Figures 1A–C, blue data-points). Finally, Hypothesis 3 predicted that choices for the Beloved would differ from those made for the Stranger, and be more similar to those observed for the Self. This was confirmed in our data, with increased risk aversion in the Beloved relative to the Stranger condition (Figures 1A–C, green data-points). In addition, participants exhibited the most risk-aversion when choosing for a loved one. The Target also affected the role played by EDS and Price on the decision, with choices for the Beloved more strongly influenced by EDS, while those for the Other were primarily price-based (Figure 2).
Finally, although our main analysis was framed on the estimation of a (dis)utility score for the disease (EDS), the results were not conditional to this choice. Similar effects were also observed when modeling the raw probability of disease contraction (pD).
3 Survey 2
In Survey 2, we explicitly differentiated risk preferences from cost concerns. For this purpose, we devised a modified version of Survey 1, where participants chose between sure and risky treatment options, and were subsequently asked to bid (in their own currency) on their chosen option. This measure of willingness-to-pay (WTP) has previously been used to valuate health interventions (Olsen and Smith, 2001). Importantly, removing the factor “price” made for a shorter survey of only 15 scenarios (5 diseases * 3 Targets). We further shortened the questionnaire to 12 scenarios (4 diseases * 3 Targets) to a survey that could be filled in ~15 min.
3.1 Methods
Unless otherwise stated, the set-up and analysis of Survey 2 were identical to those of Survey 1.
3.1.1 Population
In Survey 2, respondents were not remunerated and were recruited through social media (Facebook, Twitter and LinkedIn) and survey swapping platforms. Within a time-window of 2 months (June–July 2020), 273 participants began the survey, and 175 completed the questionnaire. Five participants were excluded from analysis for providing implausible answers, leaving a sample of n = 170 for analysis. Cohort 2 was comparable to Cohort 1 for age (of both respondents and chosen Beloved), education and number of countries represented (Table 1). However, the cohorts differed on sex ratio and income (Survey 2 included more females and respondents reported a higher income).
3.1.2 Procedure
Survey 2 included 12 scenarios with 4 diseases (Supplementary Table A1) affecting one of 3 possible targets (Self, Beloved and Stranger). Participants were asked to select between a sure option and a gamble, as in Survey 1. Respondents were not allowed to forgo action. Furthermore, no cost was associated with the options. Following choice, participants were asked to name a price [Willingness to Pay (WTP)], in their own currency for the chosen option. Respondents were explicitly told they could enter a value of 0 if they wished. Given its brevity, Survey 2 did not include any catch trials to assess attention.
3.1.3 Data analysis
As in Survey 1, we first performed a choice analysis (Model 2a) testing whether EDS, Target or their interaction affected choice. Then we examined (WTP) as a dependent variable (Model 2b), with EDS, Target, previous Choice (Gamble vs. Sure Option) and their interaction as predictors of interest (Supplementary Table A1). The WTPs were converted from participants’ local currency to USD (based on the official exchange rate on the day of their response), and log-transformed to account for the large range in responses.
Each model was associated with a power analysis to test whether the current design at a given sample size would be sufficiently powered to replicate findings from Survey 1. Estimates of fixed factors coefficients and random-effect terms for Model 2a were obtained by re-analyzing Models 1b from Survey 1 without the factor “price.” As for Model 2b, we took the coefficients/terms obtained from the analysis of treatment price (Model 1c), although this model provides only partial information as no factor “choice” was specified in Survey 1. For each model, and each main/interaction effect, we ran 1,000 Monte-Carlo simulations aimed at replicating the same fixed factors coefficients and random-effect terms observed in Survey 1 on the design and sample size from Survey 2. Power was then estimated from the frequency of significant effects from the simulated data, as implemented in the simr package of R (Green and MacLeod, 2016). This analysis showed that the design and sample size were sufficiently sensitive to replicate the effects of EDS and Target observed in Model 1b from Survey 1 with a probability of at least 0.88.
3.2 Results
3.2.1 Choice analysis
As in Survey 1, participants preferred gambles over sure options (62.72%, IQR: 25.00; test against 50%: t(169) = 6.18, p < 0.001), an effect observed in all three targets with comparable percentages. We further inspected choice preferences through a generalized linear mixed model, under binomial distribution (Model 2a). Results confirmed the same effect of EDS observed in Survey 1 (Table 4), where gambles decreased with increasing EDS (Figure 1D). We found no effect of Target. Overall, the analysis of Survey 2 revealed that when risk preferences are dissociated from cost, Target effects disappear.
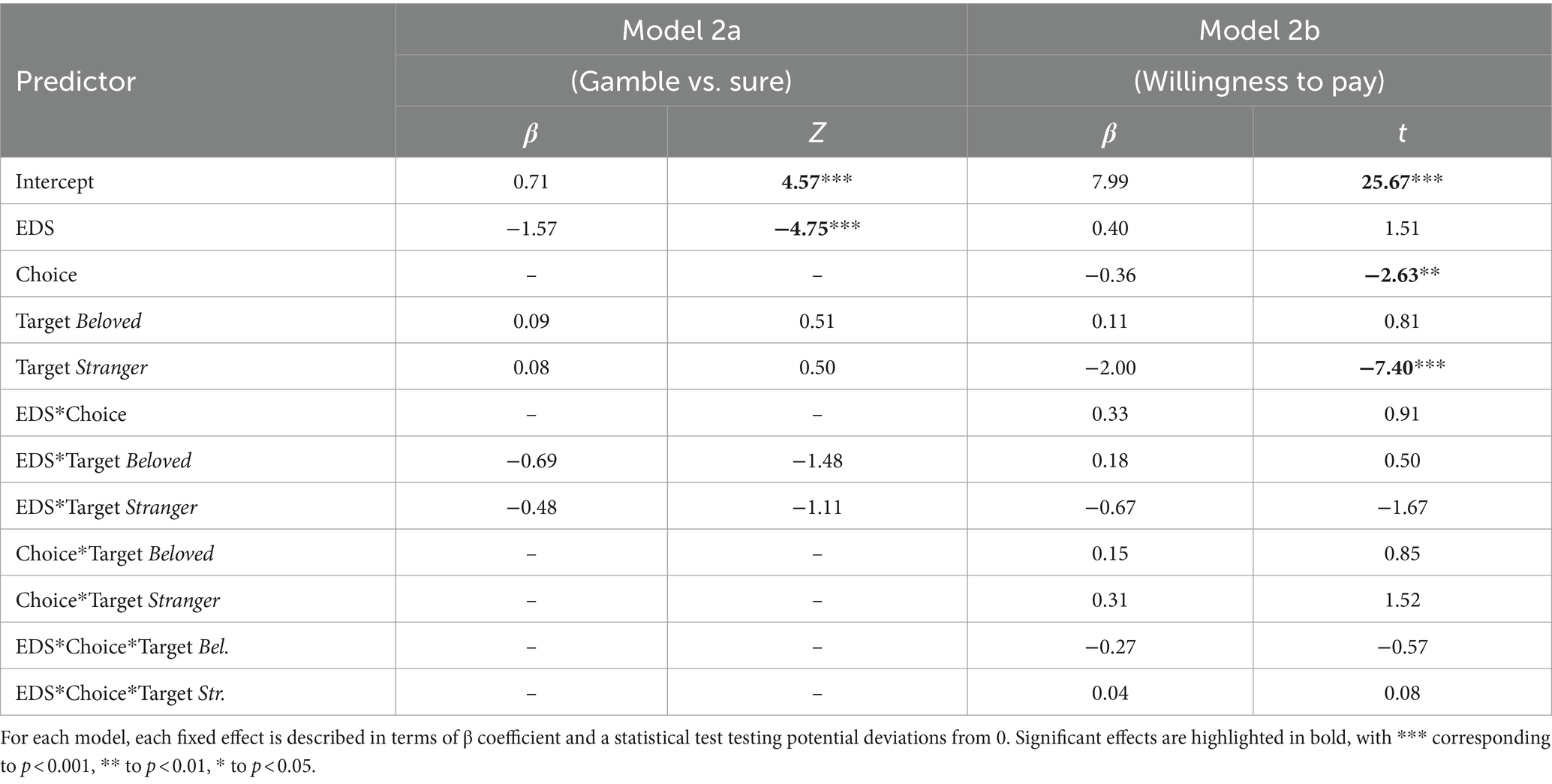
Table 4. Results of Survey 2.
3.2.2 Willingness-to-pay
In contrast to risk preferences, Target influences WTP, with participants bidding less on the Stranger (Table 4; Figure 3B). Additionally, we found an effect of previous Choice, with participants bidding more on sure options than gambles (Figure 3C). However, only 24.71% of trials listed a 0 bid for the Stranger, indicating a persistence of altruism and prosocial motivation.
3.2.3 Follow-up analyses
3.2.3.1 Nuisance variables
We repeated analyses including Sex, Age, Monthly Income and COVID-19 information as nuisance variables. Results confirmed all effects observed in the main analysis (Supplementary Table A4), with the exception of the Choice effect from Model 2c (β = −0.31, t(627.62) = −1.70, p = 0.090). When analyzing the effect of the nuisance variables, we found a significant positive effect of COVID-19 financial loss on WTP (Supplementary Figure A1), suggesting that participants who sustained a higher financial loss due to the pandemic were willing to pay more for others. This was observed by specifying both monthly income and financial loss in the same model, indicating this effect was not confounded with personal wealth.
3.2.3.2 Alternative approach to EDS
As in Survey 1, we repeated the analyses of the main models by replacing EDS with pD + SD, as two independent predictors. Full results are displayed in Supplementary Table A5, and reveal that all effects originally attributed to EDS are now associated with pD. No effect was associated with SD.
3.3 Discussion
Survey 2 confirms both Hypothesis 1 and the first result from Survey 1 in that, in the Self condition, individuals display risk-seeking behavior in the disease domain, as highlighted by the preference toward gambles vs. sure options. Furthermore, this preference for gambles decreases linearly with EDS. However, when differentiating risk preferences from cost concerns, Survey 2 results show no Target difference, going against the predictions of Hypotheses 2 and 3 (Figures 1B–D). Instead, target differences were observed only in the analysis of WTP, with participants bidding less to treat the Stranger (Figure 3B). This result disambiguates an open issue from Survey 1, suggesting target differences in other-regarding decision-making under risk are conditioned on cost considerations, and not risk preferences. Finally, while respondents preferred gambles overall, WTP analyses reveal a higher monetary value placed on sure options (Figure 3C).
4 General discussion
The goal of this study was to probe decision-making under risk in health interventions for self and others in the context of the COVID-19 pandemic’s early days. The study was specifically aimed at gaining a cross-sectional description of how a lay individual selects costly actions on behalf of another person’s health, under risk. As authorities called on the public to act for others’ sake during the pandemic, the burden of uncertain decision-making was thrust onto individual shoulders.
4.1 Individuals are risk-seeking for health treatments
Across two surveys, we confirm the first hypothesis of this study, according to which individuals prefer to gamble to prevent disease for themselves. This effect is in line with studies on different kinds of negative rewards, ranging from monetary loss (Tversky and Kahneman, 1981), to pain prevention (Loued-Khenissi et al., 2022). It is possible that the framing of decision outcomes in the present study as negative (getting sick) could have influenced the results toward a pattern similar to that of monetary losses (Tversky and Kahneman, 1981). In this perspective, an alternative framing with a positive outcome (being healed) could in principle lead to diverging results. However, surveys targeted the general population that, while in good health, was confronted with the risk of contracting COVID-19 (as the survey was conducted in the early days of pandemic, almost no-one of our participants contracted SARS-Cov-2 virus, Table 1). Casting the retention of improved health as a positive outcome in this population may have stretched responders’ credulity. This may differ in patient populations, where treatments for different disease scenarios could be realistically framed as a positive shift from their present condition.
Critically however, though participants displayed an overall preference for gambles, they became progressively more risk-averse with higher expected disease severity. This finding is consistent with previous research in the domain of economic decision-making (Tversky and Kahneman, 1981) and pain management (Loued-Khenissi et al., 2022). In addition to confirming our predictions, these results put forward the effectiveness of expected utility models in explaining health decision-making (Cohen, 1996). Although several studies criticize such an approach for health decisions (Abellan-Perpiñan et al., 2009; Dolan and Kahneman, 2008), we argue that expected utility is a useful tool for modeling individual behavior, in line with what is known on life quality (Attema et al., 2016), pain management (Loued-Khenissi et al., 2022), as well as brain activity (Knutson et al., 2005; Loued-Khenissi et al., 2020; Schultz, 2016). Importantly, our results are not idiosyncratic to the theoretical framework adopted in our study, as similar effects were obtained when replacing expected disease severity with the raw probability of disease contraction (pD). Hence, absent any explicit requests to compute probabilistic outcomes, individuals in our study appear to choose according to those quantities nonetheless. In this perspective, concerns over individuals’ difficulty in understanding probabilities, particularly in the context of the pandemic (Aguilar and Castaneda, 2021; Muñiz-Rodríguez et al., 2020) are not supported, and therefore authorities should consider informing the public in accurate, probabilistic terms (Kahlenberg et al., 2023).
Although individuals selected gambles more often, they simultaneously assigned a higher monetary value to sure treatment options (Figure 3C). This effect is known as preference reversal (Safra et al., 1990; Seidl, 2002), prevalent in economic frameworks but also observed in the domain of pain management (Loued-Khenissi et al., 2022). Although the cause of preference reversals is still debated, scholars attribute it to the sequential nature of many paradigms that distort pricing estimates, or to a general tendency to overprice options with high probability and low benefit at the expense of options with low probability and high benefit (see Seidl, 2002, for a review). Both these explanations fit the case of Survey 2, further stressing how choices in the context of disease prevention dovetail with predictions based on theories of economic decision-making.
4.2 Target differences are explained by cost considerations
In both surveys, participants’ behavior differed as a function of disease target, especially for strangers. In Survey 1, respondents selected gambles more often for strangers than for themselves or their loved ones (Figure 1C). Prima facie, these results suggest a stronger risk-seeking stance for other-regarding decisions. However, Survey 1 results may also reflect the fact that the price associated with gambles in the survey was (1) stable across trials, and (2) cheaper or equal to that of sure options. Participants’ behavior toward strangers was also characterized by a high amount of inactions (Figure 1A) where participants refrained from choosing to avoid incurring personal cost. In Survey 2, where choices were embedded in a cost-free context, individuals risk preference for others was the same as that observed for self-regarding behavior. Individuals diverged in action for themselves and unknown others only with respect to willingness-to-pay. We therefore propose that, when cost is not a factor in decision-making, risk biases do not have a differential impact on self and others. However, when cost is a factor, decisions differ between targets by pushing agents toward a value-based heuristic, where cheaper options are preferred for strangers.
It is unclear why, in the present study, risk preferences remain the same across the self-other boundary, something that contrasts with prior research that have found a dissociation (Atanasov, 2015; Loued-Khenissi et al., 2022; Polman and Wu, 2020). Two considerations emerge from this finding. First, results provide evidence that individuals deploy a simple self-referential strategy when computing uncertainty for others (at least in contexts that are cost-free and anonymous), possibly to minimize cognitive demand (Tomova et al., 2020). Second, although previous meta-analyses report overall self-other differences in risk preferences these effects are extremely variable between studies, pointing to a wide range of moderators that influence participants’ choices (Atanasov, 2015; Polman and Wu, 2020). Among these are the framing of the context (e.g., involving positive vs. negative outcomes, financial vs. medical decisions) and, most critically, the identity of the target (adult, child, patient) and his/her personal relationship with the deciding agent (family member, colleague, stranger) (Atanasov, 2015; Polman and Wu, 2020). It is possible that any of these moderating factors (or the combination thereof) might have influenced our results with respect to prior literature.
Instead, the fact that target differences (across the self-stranger boundary) emerge only when monetary cost becomes a relevant parameter to an agent is consistent with current theoretical accounts. For instance, Lockwood et al. (2017) found that effortful (costly) pro-social choices triggered apathy, thereby suggesting that one main discriminant between self vs. others decision-making lies in resource mobilization. Most importantly, these results are also in line with predictions from evolutionary theory on kinship and indirect fitness (Kay et al., 2019), according to which costly behavior might be evolutionarily advantageous only when benefiting close ones, at the expense of strangers. It should be stressed, however, that strangers still received treatments that were more expensive than the cheapest option: in Survey 1, costly choices were chosen ~48% of the time, while in Survey 2 participants consistently made bids higher than 0. Based on these results, individual behavior for strangers does not mirror self-regarding behavior—but neither does it reflect purely or even mostly selfish motivations. On the contrary, participants were willing to incur costly prosocial behavior even when kinship motives are absent, as for the stranger condition in our study. These altruistic tendencies have previously been found in several researches from behavioral economics (Fehr and Fischbacher, 2004; Fehr and Schmidt, 2006; Frey and Meier, 2004) and more generally in the field (Sisco and Weber, 2019). They offer a valuable insight into the boundaries one can expect from individuals for the sake of others’ wellbeing, especially in scenarios with high uncertainty, rather than relying on heuristics that may backfire (Bonaccorsi et al., 2020; Fink et al., 2022; Wood et al., 2022) and compromise political trust (Jørgensen et al., 2022).
It could be argued that these donations are the result of a so-called experimenter effect, where participants are motivated by reputation concerns (Hoffman et al., 1996). The experimenter effect has been observed in tasks such as the dictator game, where anonymity between the participant and the experimenters decreased the amount of free donations (Hoffman et al., 1996). However, as our study guaranteed full anonymity, we believe that the risk of such confounds are negligible. Furthermore, participants’ WTP in Survey 2 was positively influenced by real confinement-related financial loss (while controlling for personal wealth). This hints toward a genuine pro-social disposition held by respondents to provide for others’ wellbeing, including strangers. These results are in line with previous environmental research measuring willingness-to-pay for options that benefit members of a future generation. Even in those scenarios where delay-discounting can dampen pro-social motivations, people exhibit a positive attitude toward others’ wellbeing (Graham et al., 2019).
4.3 Choices for loved ones resemble those made for the self
Our third hypothesis predicted that individuals’ behavior toward a stranger would differ from that made for a loved one, in that the latter would trigger decisions more similar to those made for the self. When considering risk preferences alone, we found no target differences, thus providing no support for our prediction. However, when taking into account cost-considerations, we find evidence supporting this hypothesis. Whereas participants chose cheaper options for a stranger, the chosen cost for treating a loved one was either higher than (Survey 1) or comparable to (Survey 2) that chosen for the self. This effect is reminiscent of what is found in the literature on pain decisions, where individuals’ behavior and susceptibility to risk differs strongly between an unknown other and a loved one, with the latter resembling those made for the self (Loued-Khenissi et al., 2022). This result also conforms to the empathy model from social neuroscience literature, where individuals treat others’ suffering as their own by triggering the same neural processes that mediate direct pain experience (Bernhardt and Singer, 2012; Corradi-Dell’Acqua et al., 2011, 2016, 2023). This model acknowledges a strong role played by social proximity, with less pronounced empathic responses for those deemed distant from the self (Cheng et al., 2010; Hein et al., 2010; Xu et al., 2009).
Although similar to one another, responses associated with the self and a loved one were not identical. In particular, in Survey 1, choices made for a loved one differed in several ways from the self-condition: they were more risk averse, less influenced by price and more by EDS (or pD, depending on the analysis), and assigned a higher monetary value. These results show that social proximity shifts one’s behavior from wellbeing-oriented (for close others) to price-oriented (for strangers; see Figure 2B). These effects were not observed in Survey 2, though a power analysis established that the sample collected was adequate to reproduce Target differences from Survey 1. It is possible that these effects manifest themselves only in complex settings where price and EDS are integrated together. However, it should also be mentioned that the power analysis tested effects of Target as a whole: i.e., across all three levels. It is therefore possible that the results were influenced by the strong modulations of the Stranger condition, and that a more sensitive cohort would have been necessary to replicate subtle Self vs. Beloved differences.
4.4 Limitations of the study and future implications
This study has three limitations that need to acknowledged. First, Survey 2 different slightly from Survey 1 in that: it was shorter, it was targeted to unpaid volunteers recruited outside Prolific.co platform, and no catch trials were implemented to monitor participants’ attentional level. It is in principle possible that some participant in Survey 2 lost focus during the task despite its brevity. More critically, the two surveys might have probed slightly different populations, by attracting individuals with different financial status (Table 1). Second, recruitment for unpaid volunteers for Survey 2 was more time consuming. Given the rapid pandemic progression, it is possible that perception of risk for people’s health changed across time. Hence, a much delayed recruitment time would have exposed us to the risk of probing a different situational cohort with respect to Survey 1. We minimized such possibility by interrupting data collection following 2 months so that participants from Survey 1 (tested on May 2020) and those from Survey 2 (June–July) were tested in close proximity. The drawback of this choice was that the sample size was imbalanced between the surveys, with Survey 2 being limited to 170 participants. However, rigorous simulation-based power analysis insured that such sample was sufficiently sensitive to replicate the effects of interest from Survey 1. Third, studies on economic decision making and prosocial behavior often report big inter-individual differences, explainable in terms of personality or empathic traits (Thielmann et al., 2020), prosocial beliefs (Carlson and Zaki, 2022) as well as COVID-19 information (disease contraction, regional death rate, etc.; Fang et al., 2022). Unfortunately, personality/social traits were not collected in this study, preventing us to assess these effects also in our dataset. We did collect information about individual COVID-19 experience (see methods for the measures collected), but these measure were either unsuitable for statistical analyses (positive cases of SARS-Cov-2 virus were negligible; Table 1) or did not reveal reliable influence on choice behavior.
Keeping these considerations aside, our study provides novel and replicable evidence on how people make decisions about one’s own other people’s health under risk. In particular, we found that individuals act for their own health as is observed in the monetary loss domain, by displaying an overall risk-seeking stance that progressively declines as the expected value of a negative event increases. This effect did not differ statistically when choices under risk were made for others, at least when cost considerations were put aside. However, distinctions between decision targets emerged when choices were conditioned on monetary cost, with participants preferring cheaper treatment options for unknown others, but not for loved ones.
The COVID-19 pandemic imposed the burden of costly decision-making under risk for others’ health on ordinary people. Most of the restrictive measures implemented across the globe had negative economical, but also psychological consequences on the people involved (Kunzler et al., 2021; Lima et al., 2020; Nochaiwong et al., 2021; Santomauro et al., 2021; Wu et al., 2021). These restrictions negatively impacted sensitivity to others’ suffering, and empathy traits (Antico and Corradi-Dell’Acqua, 2023; Cao et al., 2022), thus raising the question on what cost lay individuals were willing to incur for the sake of a stranger, and this under uncertainty. In this perspective, our study provides a descriptive model of individual risky decision-making in health-contexts; and inform on the limits of what can be asked of an individual in service to a stranger. Furthermore, as global society faces looming events such as climate change (Hornsey et al., 2022) or migration (Denniston, 2021) that demand individual participation for their mitigation, it is crucial to gain an understanding of factors influencing other-regarding decision-making under uncertainty. As respondents showed a readiness to incur cost for the sake of strangers, authorities can assume a general goodwill and willingness to help others (albeit at a lower rate of cost to that observed in self-regarding decisions or decisions made for loved ones), underscoring our tendency toward pro-sociality.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found at: Open Science Framework:
Ethics statement
The studies involving humans were approved by The Ethics Committee of the Faculty of Psychology and Educational Sciences of the University of Geneva, Geneva, Switzerland. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
LL-K: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – original draft. CC-D’A: Funding acquisition, Supervision, Writing – review & editing, Conceptualization, Validation.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was funded by the Swiss National Science Foundation (SNSF) grant PP00P1_183715. CCD is further supported by SNSF grant n. 320030_182589.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at:
Footnotes
References
Abellan-Perpiñan, J. M., Bleichrodt, H., and Pinto-Prades, J. L. (2009). The predictive validity of prospect theory versus expected utility in health utility measurement. J. Health Econ. 28, 1039–1047. doi: 10.1016/j.jhealeco.2009.09.002
Crossref Full Text | Google Scholar
Adams-Prassl, A., Boneva, T., Golin, M., and Rauh, C. (2020). Inequality in the impact of the coronavirus shock: evidence from real time surveys. J. Public Econ. 189:104245. doi: 10.1016/j.jpubeco.2020.104245
Crossref Full Text | Google Scholar
Aguilar, M. S., and Castaneda, A. (2021). What mathematical competencies does a citizen need to interpret Mexico’s official information about the COVID-19 pandemic? Educ. Stud. Math. 108, 227–248. doi: 10.1007/s10649-021-10082-9
PubMed Abstract | Crossref Full Text | Google Scholar
Allais, M. (1953). Le Comportement de l’Homme Rationnel devant le Risque: Critique des Postulats et Axiomes de l’Ecole Americaine. Econometrica 21, 503–546. doi: 10.2307/1907921
Crossref Full Text | Google Scholar
Andreoni, J., and Miller, J. (2002). Giving according to GARP: an experimental test of the consistency of preferences for altruism. Econometrica 70, 737–753. doi: 10.1111/1468-0262.00302
Crossref Full Text | Google Scholar
Antico, L., and Corradi-Dell’Acqua, C. (2023). Far from the eyes, far from the heart: COVID-19 confinement dampened sensitivity to painful facial features. Q. J. Exp. Psychol. 76, 554–567. doi: 10.1177/17470218221094772
Crossref Full Text | Google Scholar
Atanasov, P. D. (2015). Risk preferences in choices for self and others: Meta analysis and research directions. SSRN scholarly paper 1682569. doi: 10.2139/ssrn.1682569
Crossref Full Text | Google Scholar
Attema, A. E., Brouwer, W. B. F., and l’Haridon, O. (2013). Prospect theory in the health domain: a quantitative assessment. J. Health Econ. 32, 1057–1065. doi: 10.1016/j.jhealeco.2013.08.006
Crossref Full Text | Google Scholar
Attema, A. E., Brouwer, W. B. F., Lharidon, O., and Pinto, J. L. (2016). An elicitation of utility for quality of life under prospect theory. J. Health Econ. 48, 121–134. doi: 10.1016/j.jhealeco.2016.04.002
Crossref Full Text | Google Scholar
Barbieri, P., and Bonini, B. (2020). Political orientation and adherence to social distancing during the COVID-19 pandemic in Italy. SSRN scholarly paper 3640324. doi: 10.2139/ssrn.3640324
Crossref Full Text | Google Scholar
Bernhardt, B. C., and Singer, T. (2012). The neural basis of empathy. Annu. Rev. Neurosci. 35, 1–23. doi: 10.1146/annurev-neuro-062111-150536
Crossref Full Text | Google Scholar
Bernoulli, D. (1738/1954). Exposition of a new theory on the measurement of risk. Econometrica 22, 23–36. doi: 10.2307/1909829
Crossref Full Text | Google Scholar
Bleichrodt, H. (1997). Health utility indices and equity considerations. J. Health Econ. 16, 65–91. doi: 10.1016/S0167-6296(96)00508-5
Crossref Full Text | Google Scholar
Bonaccorsi, G., Pierri, F., Cinelli, M., Flori, A., Galeazzi, A., Porcelli, F., et al. (2020). Economic and social consequences of human mobility restrictions under COVID-19. Proc. Natl. Acad. Sci. 117, 15530–15535. doi: 10.1073/pnas.2007658117
Crossref Full Text | Google Scholar
Boschini, A., Dreber, A., von Essen, E., Muren, A., and Ranehill, E. (2018). Gender and altruism in a random sample. J. Behav. Exp. Econ. 77, 72–77. doi: 10.1016/j.socec.2018.09.005
Crossref Full Text | Google Scholar
Cao, S., Qi, Y., Huang, Q., Wang, Y., Han, X., Liu, X., et al. (2022). Emerging infectious outbreak inhibits pain empathy mediated prosocial behaviour. Res. Square. [Preprint] (Version 2) doi: 10.21203/rs.3.rs-530170/
Crossref Full Text | Google Scholar
Cheng, Y., Chen, C., Lin, C.-P., Chou, K.-H., and Decety, J. (2010). Love hurts: an fMRI study. NeuroImage 51, 923–929. doi: 10.1016/j.neuroimage.2010.02.047
Crossref Full Text | Google Scholar
Choi, H. A., and Lee, O. E. (2021). To mask or to unmask, that is the question: facemasks and anti-Asian violence during COVID-19. J. Hum. Rights Soc. Work 6, 237–245. doi: 10.1007/s41134-021-00172-2
PubMed Abstract | Crossref Full Text | Google Scholar
Civai, C., Corradi-Dell’Acqua, C., Gamer, M., and Rumiati, R. I. (2010). Are irrational reactions to unfairness truly emotionally-driven? Dissociated behavioural and emotional responses in the ultimatum game task. Cognition 114, 89–95. doi: 10.1016/j.cognition.2009.09.001
Crossref Full Text | Google Scholar
Civai, C., Crescentini, C., Rustichini, A., and Rumiati, R. I. (2012). Equality versus self-interest in the brain: differential roles of anterior insula and medial prefrontal cortex. NeuroImage 62, 102–112. doi: 10.1016/j.neuroimage.2012.04.037
Crossref Full Text | Google Scholar
Cohen, B. J. (1996). Is expected utility theory normative for medical decision making? Med. Decis. Mak. 16, 1–6. doi: 10.1177/0272989X9601600101
Crossref Full Text | Google Scholar
Corradi-Dell’Acqua, C., Civai, C., Rumiati, R. I., and Fink, G. R. (2013). Disentangling self- and fairness-related neural mechanisms involved in the ultimatum game: an fMRI study. Soc. Cogn. Affect. Neurosci. 8, 424–431. doi: 10.1093/scan/nss014
Crossref Full Text | Google Scholar
Corradi-Dell’Acqua, C., Hofstetter, C., Sharvit, G., Hugli, O., and Vuilleumier, P. (2023). Healthcare experience affects pain-specific responses to others’ suffering in the anterior insula. Hum. Brain Mapp. 44, 5655–5671. doi: 10.1002/HBM.26468
Crossref Full Text | Google Scholar
Corradi-Dell’Acqua, C., Hofstetter, C., and Vuilleumier, P. (2011). Felt and seen pain evoke the same local patterns of cortical activity in insular and cingulate cortex. J. Neurosci. 31, 17996–18006. doi: 10.1523/JNEUROSCI.2686-11.2011
PubMed Abstract | Crossref Full Text | Google Scholar
Corradi-Dell’Acqua, C., Tusche, A., Vuilleumier, P., and Singer, T. (2016). Cross-modal representations of first-hand and vicarious pain, disgust and fairness in insular and cingulate cortex. Nat. Commun. 7:10904. doi: 10.1038/ncomms10904
Crossref Full Text | Google Scholar
Cox, J. C., and Sadiraj, V. (2008). “Risky decisions in the large and in the small: theory and experiment” in Risk aversion in experiments. eds. J. C. Cox and G. W. Harrison, vol. 12 (Bingley, UK: Emerald Group Publishing Limited), 9–40.
Google Scholar
Cutler, J., and Campbell-Meiklejohn, D. (2019). A comparative fMRI meta-analysis of altruistic and strategic decisions to give. NeuroImage 184, 227–241. doi: 10.1016/j.neuroimage.2018.09.009
Crossref Full Text | Google Scholar
Daly, M. C., Buckman, S. R., and Seitelman, L. M. (2020). The unequal impact of COVID-19: why education matters. FRBSF Econ. Lett. 17, 1–5.
Google Scholar
Denniston, L. (2021). ““They just come and try to help”: exploring the prioritization of downstream accountability in citizen-led humanitarianism in Calais” in Citizen humanitarianism at European Borders (New York, NY: Routledge), 66–82.
Google Scholar
Diekmann, A. (2004). The power of reciprocity: fairness, reciprocity, and stakes in variants of the dictator game. J. Confl. Resolut. 48, 487–505. doi: 10.1177/0022002704265948
Crossref Full Text | Google Scholar
Dolan, P., and Kahneman, D. (2008). Interpretations of utility and their implications for the valuation of health. Econ. J. 118, 215–234. doi: 10.1111/j.1468-0297.2007.02110.x
Crossref Full Text | Google Scholar
Du, R.-H., Liang, L.-R., Yang, C.-Q., Wang, W., Cao, T.-Z., Li, M., et al. (2020). Predictors of mortality for patients with COVID-19 pneumonia caused by SARS-CoV-2: a prospective cohort study. Eur. Respir. J. 55:2000524. doi: 10.1183/13993003.00524-2020
PubMed Abstract | Crossref Full Text | Google Scholar
Evans, W. N., and Viscusi, W. K. (1991). Utility-based measures of health. Am. J. Agric. Econ. 73, 1422–1427. doi: 10.2307/1242395
Crossref Full Text | Google Scholar
Fang, X., Freyer, T., Ho, C.-Y., Chen, Z., and Goette, L. (2022). Prosociality predicts individual behavior and collective outcomes in the COVID-19 pandemic. Soc. Sci. Med. 308:115192. doi: 10.1016/j.socscimed.2022.115192
Crossref Full Text | Google Scholar
Fehr, E., and Fischbacher, U. (2004). Social norms and human cooperation. Trends Cogn. Sci. 8, 185–190. doi: 10.1016/j.tics.2004.02.007
Crossref Full Text | Google Scholar
Fink, G., Tediosi, F., and Felder, S. (2022). Burden of COVID-19 restrictions: national, regional and global estimates. eClinicalMedicine 45:101305. doi: 10.1016/j.eclinm.2022.101305
PubMed Abstract | Crossref Full Text | Google Scholar
Freund, A. M., and Blanchard-Fields, F. (2014). Age-related differences in altruism across adulthood: making personal financial gain versus contributing to the public good. Dev. Psychol. 50, 1125–1136. doi: 10.1037/a0034491
Crossref Full Text | Google Scholar
Frey, B. S., and Meier, S. (2004). Pro-social behavior in a natural setting. J. Econ. Behav. Organ. 54, 65–88. doi: 10.1016/j.jebo.2003.10.001
Crossref Full Text | Google Scholar
Gollier, C., and Treich, N. (2003). Decision-making under scientific uncertainty: the economics of the precautionary principle. J. Risk Uncertain. 27, 77–103. doi: 10.1023/A:1025576823096
Crossref Full Text | Google Scholar
Graham, H., de Bell, S., Hanley, N., Jarvis, S., and White, P. C. L. (2019). Willingness to pay for policies to reduce future deaths from climate change: evidence from a British survey. Public Health 174, 110–117. doi: 10.1016/j.puhe.2019.06.001
Crossref Full Text | Google Scholar
Green, P., and MacLeod, C. J. (2016). SIMR: an R package for power analysis of generalized linear mixed models by simulation. Methods Ecol. Evol. 7, 493–498. doi: 10.1111/2041-210X.12504
Crossref Full Text | Google Scholar
Hein, G., Silani, G., Preuschoff, K., Batson, C. D., and Singer, T. (2010). Neural responses to ingroup and outgroup members’ suffering predict individual differences in costly helping. Neuron 68, 149–160. doi: 10.1016/j.neuron.2010.09.003
Crossref Full Text | Google Scholar
Hellinger, F. J. (1989). Expected utility theory and risky choices with health outcomes. Med. Care 27, 273–279. doi: 10.1097/00005650-198903000-00005
Crossref Full Text | Google Scholar
Hoffman, E., McCabe, K., and Smith, V. L. (1996). Social distance and other-regarding behavior in dictator games. Am. Econ. Rev. 86, 653–660.
Google Scholar
Hornsey, M. J., Chapman, C. M., and Oelrichs, D. M. (2022). Why it is so hard to teach people they can make a difference: climate change efficacy as a non-analytic form of reasoning. Think. Reason. 28, 327–345. doi: 10.1080/13546783.2021.1893222
Crossref Full Text | Google Scholar
Huck, S., and Müller, W. (2012). Allais for all: revisiting the paradox in a large representative sample. J. Risk Uncertain. 44, 261–293. doi: 10.1007/s11166-012-9142-8
Crossref Full Text | Google Scholar
Johnson, J. G., and Busemeyer, J. R. (2010). Decision making under risk and uncertainty. WIREs Cogn. Sci. 1, 736–749. doi: 10.1002/wcs.76
Crossref Full Text | Google Scholar
Jørgensen, F., Bor, A., Rasmussen, M. S., Lindholt, M. F., and Petersen, M. B. (2022). Pandemic fatigue fueled political discontent during the COVID-19 pandemic. Proc. Natl. Acad. Sci. 119:e2201266119. doi: 10.1073/pnas.2201266119
Crossref Full Text | Google Scholar
Kahlenberg, H., Williams, D., van Tilburg, M. A. L., and Jiroutek, M. R. (2023). Vaccine hesitancy for COVID-19: what is the role of statistical literacy? Front. Public Health 11:1230030. doi: 10.3389/fpubh.2023.1230030
PubMed Abstract | Crossref Full Text | Google Scholar
Kay, T., Lehmann, L., and Keller, L. (2019). Kin selection and altruism. Curr. Biol. 29, R438–R442. doi: 10.1016/j.cub.2019.01.067
Crossref Full Text | Google Scholar
Knutson, B., Taylor, J., Kaufman, M., Peterson, R., and Glover, G. (2005). Distributed neural representation of expected value. J. Neurosci. Off. J. Soc. Neurosci. 25, 4806–4812. doi: 10.1523/JNEUROSCI.0642-05.2005
Crossref Full Text | Google Scholar
Kunzler, A. M., Röthke, N., Günthner, L., Stoffers-Winterling, J., Tüscher, O., Coenen, M., et al. (2021). Mental burden and its risk and protective factors during the early phase of the SARS-CoV-2 pandemic: systematic review and meta-analyses. Glob. Health 17:34. doi: 10.1186/s12992-021-00670-y
Crossref Full Text | Google Scholar
Kuznetsova, A., Brockhoff, P. B., and Christensen, R. H. B. (2017). lmerTest package: tests in linear mixed effects models. J. Stat. Softw. 82, 1–26. doi: 10.18637/jss.v082.i13
Crossref Full Text | Google Scholar
Levy, M., and Nir, A. R. (2012). The utility of health and wealth. J. Health Econ. 31, 379–392. doi: 10.1016/j.jhealeco.2012.02.003
Crossref Full Text | Google Scholar
Lima, C. K. T., Carvalho, P. M. D. M., Lima, I. D. A. A. S., Nunes, J. V. A. D. O., Saraiva, J. S., De Souza, R. I., et al. (2020). The emotional impact of coronavirus 2019-nCoV (new coronavirus disease). Psychiatry Res. 287:112915. doi: 10.1016/j.psychres.2020.112915
PubMed Abstract | Crossref Full Text | Google Scholar
Lockwood, P. L., Hamonet, M., Zhang, S. H., Ratnavel, A., Salmony, F. U., Husain, M., et al. (2017). Prosocial apathy for helping others when effort is required. Nat. Hum. Behav. 1:0131. doi: 10.1038/s41562-017-0131
PubMed Abstract | Crossref Full Text | Google Scholar
Lorettu, L., Piu, D., and Bellizzi, S. (2021). “Uncertainty in pandemic times” in Anxiety, uncertainty, and resilience during the pandemic period—anthropological and psychological perspectives (London, UK: IntechOpen).
Google Scholar
Loued-Khenissi, L., Martin-Brevet, S., Schumacher, L., and Corradi-Dell’Acqua, C. (2022). The effect of uncertainty on pain decisions for self and others. Eur. J. Pain 26, 1163–1175. doi: 10.1002/ejp.1940
Crossref Full Text | Google Scholar
Loued-Khenissi, L., Pfeuffer, A., Einhäuser, W., and Preuschoff, K. (2020). Anterior insula reflects surprise in value-based decision-making and perception. NeuroImage 210:116549. doi: 10.1016/j.neuroimage.2020.116549
Crossref Full Text | Google Scholar
Loued-Khenissi, L., and Preuschoff, K. (2020). Information theoretic characterization of uncertainty distinguishes surprise from accuracy signals in the brain. Front. Artif. Intell. 3:5. doi: 10.3389/frai.2020.00005
PubMed Abstract | Crossref Full Text | Google Scholar
McKee, M., and Stuckler, D. (2020). If the world fails to protect the economy, COVID-19 will damage health not just now but also in the future. Nat. Med. 26, 640–642. doi: 10.1038/s41591-020-0863-y
Crossref Full Text | Google Scholar
Meltzer, D. (2001). Addressing uncertainty in medical cost–effectiveness analysis: implications of expected utility maximization for methods to perform sensitivity analysis and the use of cost–effectiveness analysis to set priorities for medical research. J. Health Econ. 20, 109–129. doi: 10.1016/S0167-6296(00)00071-0
Crossref Full Text | Google Scholar
Muñiz-Rodríguez, L., Rodríguez-Muñiz, L. J., and Alsina, Á. (2020). Deficits in the statistical and probabilistic literacy of citizens: effects in a world in crisis. Mathematics 8:1872. doi: 10.3390/math8111872
Crossref Full Text | Google Scholar
Nochaiwong, S., Ruengorn, C., Thavorn, K., Hutton, B., Awiphan, R., Phosuya, C., et al. (2021). Global prevalence of mental health issues among the general population during the coronavirus disease-2019 pandemic: a systematic review and meta-analysis. Sci. Rep. 11:10173. doi: 10.1038/s41598-021-89700-8
PubMed Abstract | Crossref Full Text | Google Scholar
Olsen, J. A., and Smith, R. D. (2001). Theory versus practice: a review of ‘willingness-to-pay’ in health and health care. Health Econ. 10, 39–52. doi: 10.1002/1099-1050(200101)10:1<39::AID-HEC563>3.0.CO;2-E
PubMed Abstract | Crossref Full Text | Google Scholar
Pinto-Prades, J. L., Attema, A., and Sánchez-Martínez, F. I. (2019). “Measuring health utility in economics” in Oxford Research Encyclopedia of Economics and Finance.
Google Scholar
Polman, E., and Wu, K. (2020). Decision making for others involving risk: a review and meta-analysis. J. Econ. Psychol. 77:102184. doi: 10.1016/j.joep.2019.06.007
Crossref Full Text | Google Scholar
Reis, J., and Spencer, P. S. (2019). Decision-making under uncertainty in environmental health policy: new approaches. Environ. Health Prev. Med. 24:57. doi: 10.1186/s12199-019-0813-9
Crossref Full Text | Google Scholar
Ruggeri, K., Alí, S., Berge, M. L., Bertoldo, G., Bjørndal, L. D., Cortijos-Bernabeu, A., et al. (2020). Replicating patterns of prospect theory for decision under risk. Nature human. Behaviour 4, 622–633. doi: 10.1038/s41562-020-0886-x
Crossref Full Text | Google Scholar
Russell, L. B., and Schwartz, A. (2012). Looking at patients’ choices through the lens of expected utility: a critique and research agenda. Med. Decis. Mak. 32, 527–531. doi: 10.1177/0272989X12451339
Crossref Full Text | Google Scholar
Safra, Z., Segal, U., and Spivak, A. (1990). Preference reversal and nonexpected utility behavior. Am. Econ. Rev. 80, 922–930.
Google Scholar
Samuelson, P. A. (1993). Altruism as a problem involving group versus individual selection in economics and biology. Am. Econ. Rev. 83, 143–148.
Google Scholar
Santomauro, D. F., Mantilla Herrera, A. M., Shadid, J., Zheng, P., Ashbaugh, C., Pigott, D. M., et al. (2021). Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet 398, 1700–1712. doi: 10.1016/S0140-6736(21)02143-7
Crossref Full Text | Google Scholar
Soetevent, A. R. (2005). Anonymity in giving in a natural context—a field experiment in 30 churches. J. Public Econ. 89, 2301–2323. doi: 10.1016/j.jpubeco.2004.11.002
Crossref Full Text | Google Scholar
Sunstein, C. R. (2005). The precautionary principle as a basis for decision making. Econ. Voice 2, 1–9. doi: 10.2202/1553-3832.1079
Crossref Full Text | Google Scholar
Taylor, S., and Asmundson, G. J. G. (2021). Negative attitudes about facemasks during the COVID-19 pandemic: the dual importance of perceived ineffectiveness and psychological reactance. PLoS One 16:e0246317. doi: 10.1371/journal.pone.0246317
Crossref Full Text | Google Scholar
Thielmann, I., Spadaro, G., and Balliet, D. (2020). Personality and prosocial behavior: a theoretical framework and meta-analysis. Psychol. Bull. 146, 30–90. doi: 10.1037/bul0000217
Crossref Full Text | Google Scholar
Tomasello, M., Melis, A. P., Tennie, C., Wyman, E., and Herrmann, E. (2012). Two key steps in the evolution of human cooperation: the interdependence hypothesis. Curr. Anthropol. 53, 673–692. doi: 10.1086/668207
Crossref Full Text | Google Scholar
Tomova, L., Saxe, R., Klöbl, M., Lanzenberger, R., and Lamm, C. (2020). Acute stress alters neural patterns of value representation for others. NeuroImage 209:116497. doi: 10.1016/j.neuroimage.2019.116497
Crossref Full Text | Google Scholar
Tversky, A., and Kahneman, D. (1981). The framing of decisions and the psychology of choice. Science 211, 453–458.
Google Scholar
Tversky, A., and Kahneman, D. (1992). Advances in prospect theory: cumulative representation of uncertainty. J. Risk Uncertain. 5, 297–323. doi: 10.1007/BF00122574
Crossref Full Text | Google Scholar
Wiepking, P., and Breeze, B. (2012). Feeling poor, acting stingy: the effect of money perceptions on charitable giving. Int. J. Nonprofit Volunt. Sect. Mark. 17, 13–24. doi: 10.1002/nvsm.415
Crossref Full Text | Google Scholar
Wood, R., Reinhardt, G. Y., Rezaeedaryakenari, B., and Windsor, L. C. (2022). Resisting lockdown: the influence of COVID-19 restrictions on social unrest. Int. Stud. Q. 66:sqac015. doi: 10.1093/isq/sqac015
Crossref Full Text | Google Scholar
Wu, T., Jia, X., Shi, H., Niu, J., Yin, X., Xie, J., et al. (2021). Prevalence of mental health problems during the COVID-19 pandemic: a systematic review and meta-analysis. J. Affect. Disord. 281, 91–98. doi: 10.1016/j.jad.2020.11.117
Crossref Full Text | Google Scholar
Xu, X., Zuo, X., Wang, X., and Han, S. (2009). Do you feel my pain? Racial group membership modulates empathic neural responses. J. Neurosci. 29, 8525–8529. doi: 10.1523/JNEUROSCI.2418-09.2009
Crossref Full Text | Google Scholar
link